Social determinants of health (SDoH)—the conditions in which people live and the systems that shape those conditions—are increasingly receiving attention. The COVID-19 pandemic, by exacerbating inequities and highlighting the prevalence of unmet basic needs,1 has accelerated efforts to address SDoH.2 State Medicaid agencies, payers, providers, vendors, community-based organizations (CBOs), and other stakeholders have taken up the torch and are laying the foundations for long-term SDoH programs (see sidebar “What are social determinants of health?”).
Despite the momentum, however, many stakeholders across the ecosystem are still in the early stages of addressing patients’ SDoH sustainably and at scale. Stakeholders largely cite funding as the largest barrier to real progress.3 Many stakeholders know of available funding for delivering services such as food assistance, housing support, and transportation. However, options for funding data, analytics, and technology infrastructure that can optimize efforts to deliver services are less well-known. But this funding does indeed exist. And it can be used to support data integration (collating social-needs data alongside clinical and other data) and screening and referral capabilities (business processes and capabilities that include SDoH data sets to drive enrollment into targeted case management profiles for patients’ risk profile).
In pursuing these programs and seeking to secure funding, coordination across stakeholders may be crucial. SDoH is cut across a variety of focus areas and could be addressed better by working across payers, providers, states, communities, and other local actors and agencies. SDoH vendors can work alongside states and other entities to identify these funding possibilities and unify disparate stakeholders to unlock financial assistance, potentially resulting in evidence-based solutions across systems, clinical departments, and programs—and, ultimately, increased impact (see sidebar “Federal funding opportunities for actors that address social determinants of health”).
This article describes four federal financing mechanisms that are available to support SDoH data and analytics efforts and considerations for accessing them. While these insights primarily focus on possibilities for state Medicaid agencies, there are implications and potential opportunities for stakeholders across the ecosystem. This analysis is not exhaustive; rather, it provides a helpful starting point for planning and forming partnerships to support SDoH.
Four federal-funding channels are available for SDoH infrastructure efforts
Stakeholders can consider four federal-funding channels to advance their SDoH goals: waivers and authorities, federal agencies and programs, emerging opportunities resulting from recent legislation, and managed-care standards and support. Some of these federal channels provide ongoing support, for example, through a federal match or reimbursement strategy, while others provide one-time support such as through grants (see sidebar “Definitions of funding terms”). Local- or state-level and private or philanthropic funding, while not evaluated in this article, may provide additional funding opportunities for stakeholders to consider.
1. Waivers and authorities
Although federal Medicaid funds are traditionally used to cover the costs of medical services, a variety of waivers and authorities have added flexibility so these funds can cover nonmedical services outside of the Medicaid state plan—such as case management, food support, and housing support—that contribute to health outcomes (Exhibit 1). This added flexibility may also cover data and analytics infrastructure to help improve how SDoH services are delivered and the outcomes of these services on people’s lives.4 The Centers for Medicare & Medicaid Services (CMS) articulated a number of these waivers, authorities, and other supports available to address SDoH in a letter to state health officials in 2021.5 More recently, the Medicaid and CHIP Payment and Access Commission (MACPAC) released an issue brief on SDoH financing strategies.6

While waivers and authorities primarily fund direct-service delivery authorities, states often have flexibility in the proposals they put forth through waivers—for example, they may define their own demonstration project or pilot for an 1115 waiver. But waivers also often include guidelines—such as demanding budget neutrality or that a project demonstrates value in terms of quality and cost to the Medicaid program—to ensure consistency in desired outcomes.7 Federal matches from Medicaid waivers and authorities, as well as grants from the Centers for Medicare & Medicaid Innovation Center (CMMI), are among the most commonly used federal-funding sources for state Medicaid agencies to support SDoH data and programming efforts to date (see sidebar “How California and North Carolina have harnessed waivers to advance SDoH data and technology infrastructure”).
2. Federal programs and agencies
Federal programs and agencies encompass sources that regularly fund state Medicaid agencies and have supported SDoH and data and analytics infrastructure efforts, as well as sources that support SDoH efforts but are not commonly known for funding state Medicaid agencies (Exhibit 2).

Traditional state Medicaid support. Traditional-funding sources that state Medicaid agencies can access come from both the CMMI and the Medicaid Enterprise System (MES) through the Center for Medicaid and CHIP Services (CMCS). CMMI provides grants to test modified payment approaches and, at times, offers specific grants to support SDoH initiatives. For example, CMMI’s past Accountable Health Communities Model grants linked Medicare and Medicaid beneficiaries to community services with funding for screening social needs, referrals, and care navigation.8 Additional SDoH-related funding opportunities are likely to arise from CMMI given that it prioritizes health equity as a core strategic objective and addressing SDoH can help achieve this equity.9
CMCS MES approval, by comparison, is an ongoing funding source to advance Medicaid infrastructure and technology. CMCS MES funding is commonly used by states to build broader data and infrastructure but has to date been a largely untapped source for SDoH data and infrastructure capability-building (see sidebar “An in-depth look at CMCS MES funding”).
Funding from other government programs and agencies. Other federal programs and agencies whose missions align with SDoH-related priorities, such as the Health Resources and Services Administration, Department of Housing and Urban Development, and Department of Agriculture, among others, present additional potential federal-funding sources. Stakeholders may be able to codevelop SDoH data and referral solutions by considering potential flexibility under block grants (that is, grants from a federal to local authority, often with flexibility for use) or through partnerships with other organizations that commonly receive funding from these sources—such as cities, counties, local public-health departments, and not-for-profits.
Others have set the precedent of using funding from these sources for SDoH-related technological support. For example, 211 San Diego is a not-for-profit organization connecting individuals with community, health, and disaster services. With a mix of corporate, foundation, and government resources—including US Department of Agriculture (USDA) resources supporting referral-related technology—it has developed a mobile application that gives users updates as they progress in the process of finding community services.10
Other agencies, such as the CDC, have historically been less traditional sources for state Medicaid support but may present a greater opportunity going forward. Indeed, the CDC is forecasting an investment of roughly $4 billion through grants for strengthening US public-health infrastructure, workforce, and data systems that may be open to entities such as state and local governments.11
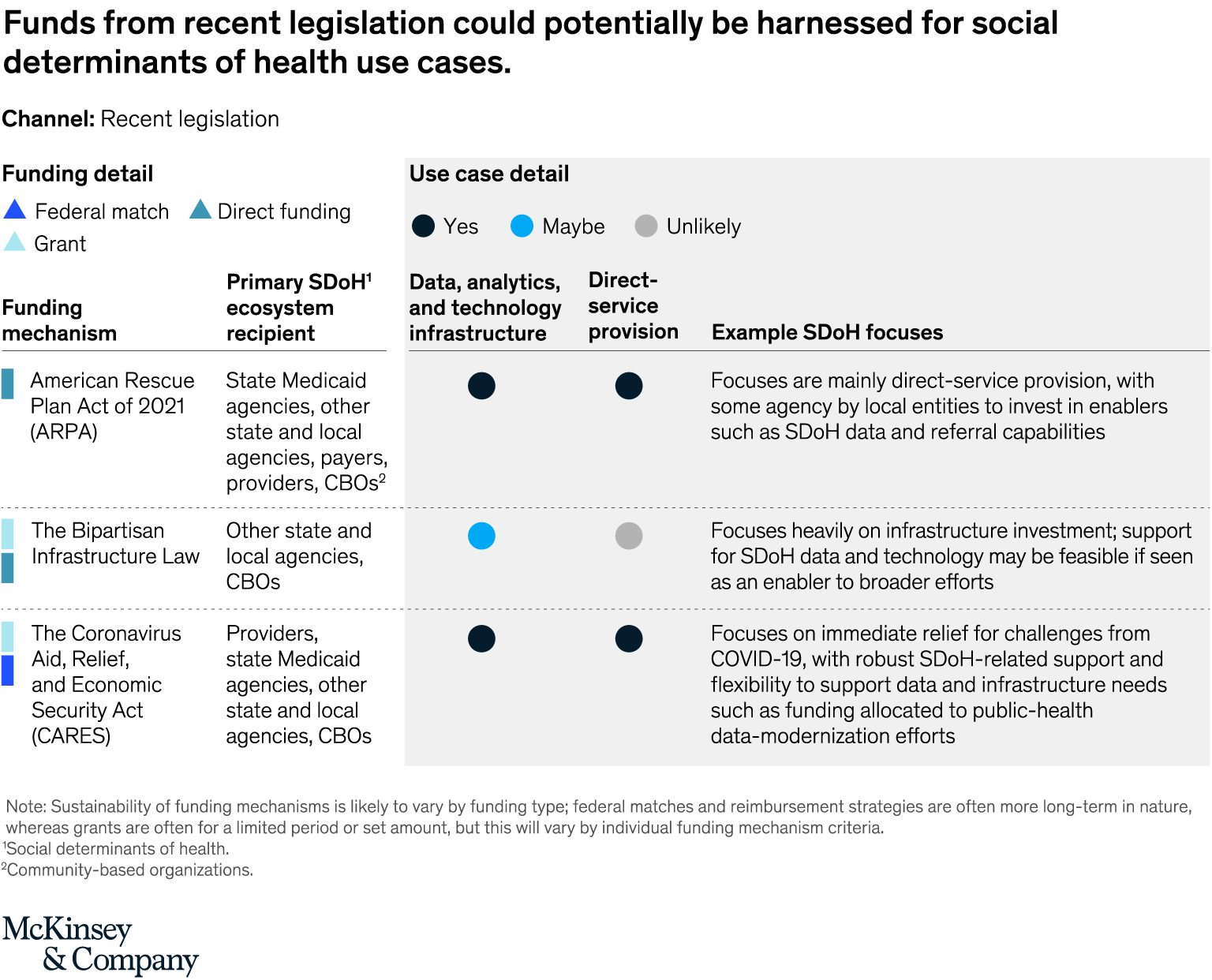
3. Recent legislation
Recent laws such as the American Rescue Plan Act (ARPA) and the Bipartisan Infrastructure Law have increased the federal funding available to support SDoH-related efforts. This legislation is providing direct food and housing supports as well as investments in data modernization and infrastructure. For example, it was announced that funding from ARPA would also support the CDC’s public health infrastructure, workforce, and data modernization efforts.12
Much of this funding will be seen through the federal programs and sources listed above, and SDoH stakeholders can watch for future grants and related opportunities from these new resources. An example of this is the inclusion of the Digital Equity Act in the Bipartisan Infrastructure Law, which allocates $2.75 billion over five years to address, for example, broadband infrastructure to improve healthcare outcomes in underserved communities (Exhibit 3).13
4. Managed-care standards and support
There is potential to unlock funding for SDoH through standards and supports related to managed care (Exhibit 4). Managed care—a funding model through which payments are per patient rather than per service, with varying degrees of financial risk—is not itself a federal funding mechanism. But states can access federal support through federal grant initiatives related to managed care. For example, CMS alternative payment model innovation funding, such as past State Innovation Model (SIM) grants, are related to managed care (see sidebar “How Michigan used SIM funding and MCO requirements to advance SDoH infrastructure”). The SIM initiative provided federal support for states advancing multipayer healthcare payment and delivery system reform models to achieve better quality of care, improve care outcomes, and deliver lower costs.14 States may continue to look for future CMMI grants focused on advancing managed care and innovative payment models to unlock SDoH data and potential infrastructure support.

Stakeholders can also take note of federal standards that can affect managed care, such as medical loss ratio (MLR) inclusion regulations.15 MLR is a financial measurement defined by CMS that looks to demonstrate and ensure value for beneficiaries. This value is measured by quality improvement activities to improve healthcare outcomes, including wellness and SDoH.16 Linking SDoH investments to quality improvement may help states unlock additional support.
Beyond these federal supports, states have the flexibility to encourage innovation in SDoH across managed-care organizations (MCOs). For example, MCOs can use value-added services and “in lieu of” services to provide services that may include SDoH-related benefits; states may also use procurement, contracts, and performance management across MCOs to encourage SDoH-related innovations.17
Potential actions to advance SDoH infrastructure efforts
Across funding mechanisms, states may consider eight actions to build on the current momentum around and increase emphasis on health equity and SDoH to advance SDoH data and technology infrastructure efforts and potentially capture the full value of available funding channels.
Integrating SDoH into broader strategic priorities. To unlock federal support for SDoH, states, vendors, payers, providers, and others are increasingly highlighting that SDoH is integral to broader strategic priorities across organizations rather than a one-off project. For the Medicaid program, for example, addressing SDoH could be part of the strategy to improve individual and population-level outcomes and to lower care delivery costs.
Articulating how SDoH data and infrastructure is a critical enabler. In addition to integrating SDoH into broader strategic priorities, stakeholders may wish to emphasize the importance of SDoH data, technology, and infrastructure as an enabler to unlocking the value from SDoH. For example, data provides insight into who has unmet basic needs, and a referral platform can allow individuals to be connected to timely interventions that improve health outcomes. Emphasizing the role of SDoH data, technology, and infrastructure in enabling these efforts may support states and other stakeholders in accessing less-traditional funding mechanisms for this purpose.
Bridging the gap between IT or data programs and service-delivery programs. To foster greater coordination and impact, IT and service delivery departments could work in tandem, recognizing the value SDoH data and technology can have in accelerating and improving service delivery efforts.
Partnering and combining funding mechanisms. Stakeholders may consider combining or sequencing funding mechanisms—from multiple federal sources as well as state, local, private, and other sources—to potentially unlock greater resourcing and ensure sustainability. For example, if a state receives an 1115 waiver to advance SDoH data and technology, it may also pursue CMCS MES funding to advance the effort. To effectively streamline funding across partners, stakeholders may consider how to collaborate and work on joint efforts with a deliberate approach to cooperative governance. This partnership or coalition-based approach may unlock greater access to disparate funding mechanisms and ensure greater alignment across the SDoH ecosystem (Exhibit 5).
Expanding target beneficiary populations. Stakeholders could also consider steps to expand SDoH efforts to a variety of beneficiary populations, such as pregnant women and children, as SDoH data and technology enables a deeper understanding of needs and a greater reach with efforts. For example, closed-loop referrals can support a vast array of patients. This may also support states and other stakeholders in accessing less-traditional funding sources, such as from government agencies.
Evaluating governance and capability gaps. Across funding sources, clear programming governance and a strong understanding of current state data and technology capabilities and gaps could be key to success in SDoH efforts.
Assessing approaches to implement SDoH infrastructure. Stakeholders may consider approaches such as Medicaid contracting, MCO requirements and MLR allowances, health information exchange (HIE) partnerships, and department-specific initiatives to implement SDoH technology and infrastructure.
Considering how data is gathered and retained, stakeholders may also want to consider what types of data and data collection and transmission standards are required to support SDoH in the context of interoperability. As conversations on interoperability continue, stakeholders will likely need discussions on data ownership, data systems of truth, and how the data is used in a way that optimizes and contextualizes care delivery and outcomes that drives holistic impact for an individual.
Stakeholders across the broader healthcare ecosystem can come together and build on the momentum currently surrounding SDoH to potentially unlock transformational impact for patients and communities while also contributing to improved healthcare and economic productivity. Although numerous federal-funding possibilities are available in silos, a collaborative or partner-driven strategy—in which human services, Medicaid, and other stakeholders work together to use their relevant funding mechanisms to support the needs of their shared beneficiaries—could potentially boost the impact of SDoH efforts. This collaboration could encourage data sharing that may transform stakeholders’ understanding of unmet basic needs, including how to address them.
Legal disclaimer: These materials do not constitute legal, medical, policy, or other regulated advice. The recipient remains solely responsible for all decisions, use of these materials, and compliance with applicable laws, rules, regulations, and standards.


