Two interrelated factors—the growing prevalence of chronic diseases and population aging—are placing a heavy burden on health systems. In all parts of the world except Africa, chronic diseases are by far the leading cause of death and disability, and they now account for 75 percent of global health care spend (an amount that is likely to increase in coming years).1 Furthermore, in almost every country, the proportion of people age 60 or older is growing far faster than any other age group, a result of both longer life expectancy and declining fertility rates.2 As people grow older, they are more apt to suffer from chronic diseases, but aging alone can increase their frailty—and their need for health care.
If the health care needs of the chronically ill and elderly are not adequately addressed, the consequences for both patients and health systems could be severe. The failure to appropriately manage disease often leads to worsening patient health; the failure to provide patients with carefully coordinated care can allow small problems to escalate into medical emergencies. Both scenarios can result in unnecessary hospitalizations, increased mortality, and higher health system costs.
Although the consequences of providing inadequate care to these groups are well known, most health systems have found it difficult to address their needs appropriately, in part because care delivery is often fragmented. Poor communication between general practitioners and specialists, for example, can hinder effective chronic disease management; some components of care may be duplicated, whereas others may be overlooked. The absence of a good interface between the health system and social services can allow elderly patients to “fall through the cracks” because neither side understands the full extent of the patients’ problems. Care fragmentation also frustrates patients, who find it difficult to navigate among the various providers and often feel that there is no one person who can help them get all essential services.
Although closer care integration offers patients significant benefits, it is hard for most health systems to provide. To date, only a few organizations around the world have found ways to integrate care effectively and thereby offer the coordinated management that chronically ill and elderly patients require. We have spoken with these organizations (individually and in panels) to learn from their experience and identify best practices. In this article, we have summarized our findings as a way to help other groups that want to pilot or improve their integrated-care programs.
What integrated care is—and is not
Integrated care brings together the different groups involved in patient care so that, from the patient’s perspective, the services delivered are consistent and coordinated. Too often, providers focus on single episodes of treatment, rather than the patient’s overall well-being. By taking a more comprehensive approach, integrated care offers patients higher-quality, more efficient care that better meets their needs. In many cases, the increased efficiency also helps control costs.
Different approaches have been used to integrate care, but they share this trait: they design all stages of care delivery around what is best for patients. The approaches can be grouped into three broad categories:
Integration between primary care and secondary care. These efforts are usually designed to provide “one stop shop” services for patients; to improve care coordination, especially for people requiring long-term care (who, by definition, include chronically ill and elderly patients); or to ensure more appropriate use of health care resources. Polikum, the largest provider of integrated outpatient health services in Germany, exemplifies this approach. Its guiding philosophy is that patients should be able to obtain all types of outpatient care under one roof. At its polyclinics in Berlin, patients can consult primary care physicians, specialists, nutritionists, and other health professionals; they can also undergo diagnostic tests and have prescriptions filled. Polikum executives have estimated that within a year of adopting this approach, the company’s hospitalization costs were reduced by about half.3
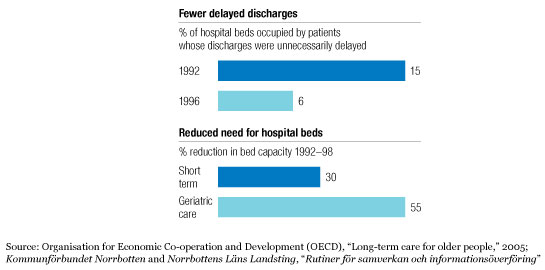
Integration between health care and community care. These efforts coordinate a wider range of services, including social services and community nursing services. Sweden took the lead in this area more than a decade ago. For example, before an elderly or disabled patient can be discharged from a Swedish hospital (to go home or to a lower-acuity care setting), a physician from the hospital and a case worker from the municipal social services agency must jointly develop a plan to ensure that the patient will receive appropriate follow-up services. This has enabled the country to improve the care delivered to these patients and, at the same time, to reduce the number of patients kept in the hospital once they no longer need high-acuity treatment (Exhibit 1).
Faster patient discharges
Integration between payors and providers. These efforts are designed to more closely coordinate care planning, commissioning, and delivery. Payor-provider integration also makes it easier to ensure that the incentives within the system encourage all providers to maximize care quality while minimizing cost. Kaiser Permanente has taken advantage of its integrated payor and provider functions to provide better care for patients who have suffered an acute coronary event. It is able to identify all such patients and offer them closely coordinated follow-up care. The program has decreased the need for costly emergency interventions and significantly reduced the risk of death.4
Questions to ask when piloting integrated care
Integration is a means to an end, not an end in itself. Therefore, any organization that wants to pilot an integrated-care program must be clear about why it is conducting the pilot and what it hopes to accomplish. The organization must also be realistic about what it can achieve in any one pilot, and thus it should focus on where it can have the greatest impact. Even the organizations that are best at providing integrated care did not attempt initially to integrate every aspect of health and social care.
The five questions below can help an organization identify where it can have the biggest impact and what it needs to do to achieve that impact. There are no “right” answers to these questions; decisions should be based on the needs of the community and the context within which the organization is operating. In all five cases, a range of answers is possible.
1. Which patients and clinical pathways should be integrated?
The answer to this question can be narrow, expansive, or somewhere in between. For example, one organization might opt to start with a single clinical pathway; another might be more ambitious, wanting to include all patients in need of long-term care. Some organizations might decide to steer a middle course, focusing on all patients who use specific types of services (for example, home nursing care).
A narrow approach is best if the goal is to optimize health outcomes in a specific patient population. This was the case when Bolton Primary Care Trust in the United Kingdom decided to build a diabetes network to address the region’s high prevalence of that disease. The network, which includes primary care, secondary care, social services, volunteer groups, and patient representatives, has enabled Bolton to ensure that diabetes patients get high-quality care from well-trained local teams. Similarly, many payors in Germany are using integrated disease-management programs to improve care delivery to patients with specific conditions (diabetes, heart disease, and asthma, for example).
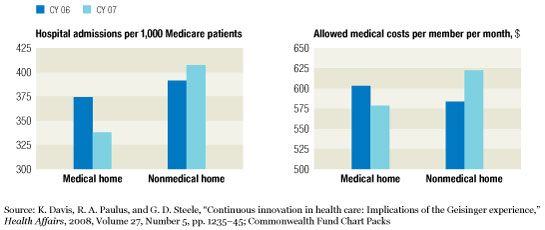
In contrast, Geisinger Health System in the United States wanted to optimize the health of all patients with chronic conditions. It therefore inaugurated its medical home program, which includes round-the-clock primary and specialty care access, a nurse care coordinator at every private provider site, and home-based monitoring. Preliminary data indicate that this program has reduced hospitalization rates and medical costs significantly (Exhibit 2).5
Lower hospital admissions and costs
2. How many people should be included?
The scale of the effort will depend on the clinical pathways selected for the pilot. Thus, the population included can be anywhere from a few thousand people to hundreds of thousands.
Both the project’s financial viability and its clinical viability must be considered. If a large investment is required for a small population, the benefit to be achieved should be fairly significant. Otherwise, it may be wiser to focus the pilot on a problem affecting a larger population to increase the return on the investment.
In some cases, however, the local community may not be large enough to make certain forms of integrated care clinically viable. For example, integrated care can benefit children with chronic renal failure. Studies have shown, though, that the medical expertise and equipment needed to provide high-quality care for these children will be cost-effective only if the local population contains at least 500,000 people.6 If the local population is smaller, there will not be a sufficient number of children to treat. In this case, it would be far better for the organization to contract with a larger nearby provider than to attempt to integrate care for these children on its own.
3. Which services should be included?
The answers to the two previous questions determine which professionals need to be involved. For example, if the primary goal is to improve the management of chronic conditions by minimizing hospital admissions and maximizing care delivered in the community, then primary care physicians, specialists, home nursing services, and perhaps other community-based health professionals will have to be included. If, however, the aim is to provide fully coordinated care for elderly patients, then social support services and sometimes other agencies will also need to be involved.
As the decision about which services to include is made, a key consideration is whether payors should also be involved. Payor participation is not a requirement, but it can help ensure that all incentives are appropriately aligned. In Germany, for example, the public payor AOK has used incentives to strengthen coordination among GPs, hospitals, and nursing homes and thereby improve the services delivered to elderly patients.
4. Which model of integration should be used?
Here, there are basically two choices: structural and virtual. Structural integration requires that different organizations either be merged or have some sort of formal partnership or joint-venture arrangement. Virtual integration requires only that the organizations work closely together. In both cases, the best results are achieved when effective governance mechanisms, including strong performance management, are in place.
The Veterans Health Administration (VHA) is a good example of the value of structural integration. VHA, the largest integrated health care organization in the United States, delivers a wide range of health services to retired military personnel. It outranks many other US providers in the quality of care it delivers, the outcomes it achieves, and the efficiency of its care delivery.7
However, full integration into a single organization is not a necessity. In some countries, physicians in private practice have banded together to form independent practice associations (IPAs). These associations help physicians in their negotiations with payors; in addition, they encourage collaboration and increased efficiency in care delivery. The physicians remain autonomous, but the IPAs give them incentives to coordinate care.
When the model of integration is being selected, a key issue to consider is what minimum requirements must be in place for the experiment to succeed. Can a virtual model provide strong enough incentives for cooperation, or is structural integration required for effective governance? Pragmatically, structural integration is not always possible. When this is the case, the organization should put other governance mechanisms in place to ensure that care is coordinated.
5. What other organizational enablers are needed?
Five factors can help maximize the results obtained with integrated care:
Patient self-care. Integrated care achieves best results when patients take control of their own health—when they actively manage their own care, avoid unhealthy behaviors, and can accurately identify when they need clinical intervention. Having patients take responsibility for their own care helps ensure that they do not inadvertently undermine the efforts of the integrated-care team. Incentives (discounts on gym memberships, for example) help motivate patients to make the necessary changes. In addition, patients must also be given information, support, and tools they can use to manage their condition (for example, visual-management tools that enable them to see their targets and track their progress).8
Team responsibilities and accountability (the “panel approach”). Integrated care is provided by a team of professionals who must work together to deliver the necessary services. For the team to function effectively, there must be clarity about who is responsible for what. If possible, a single person should have ultimate accountability for each patient; this helps ensure that all appropriate services are delivered but no duplicate or unnecessary services are ordered. However, a single point of accountability may not always be possible, especially when integration is virtual. In such cases, all care providers need to understand what they are accountable for, develop and then agree to follow protocols for how care will be delivered, and communicate regularly with other team members.
Information infrastructure (a “registry”). High-quality, efficient care and information sharing are possible only if all care providers have easy access to up-to-date patient records; they must also be able to update those records easily. This type of functionality is best provided through a strong information system. Electronic patient records do more than improve care during individual patient visits; they also make it easier to plan for future care needs, because they enable more accurate risk profiling and predictive modeling of which patients are likely to require the most attention. Reliable, real-time information also facilitates more robust performance management.
Clinical leadership. If changes in health care delivery are to succeed, it is crucial that clinicians (especially physicians) play a prominent role. They must learn to see themselves not only as the professionals who deliver patient care but also as partners in—and, ideally, leaders of—the change effort. For this to occur, they will have to be convinced of the need for integrated care and accept responsibility for seeing that the necessary changes are implemented. Once this attitudinal shift takes place, the clinicians should be encouraged to act as role models for others. Those who want to assume leadership roles should be given appropriate training and additional compensation.
Governance and provider incentives. An integrated-care pilot must be predicated on a strong vision—a clear understanding of what the project’s goal is and how that goal will be achieved. In addition, the project must have a clear governance structure; either a single board should be in charge of the effort or the involved organizations should have an agreed-upon plan for how decisions will be made. Everyone involved in the project must understand that their responsibilities will be defined and their performance—as well as the success of the overall effort—will be monitored and measured. Incentives (both financial and nonfinancial) should be offered to all participants to encourage improved care quality and increased productivity.
Ideally, all of these factors should be in place if the integration effort is to maximize its ability to improve outcomes and reduce costs. However, which of these factors are most important to the success of the effort will depend on the pilot being conducted and the setting in which that pilot takes place. For example, when Knappschaft, Bahn, See, a German payor and hospital system, decided to implement clinical pathways as a way to integrate care and thereby improve its quality and cost-efficiency, it focused first on getting physicians’ support by having them help develop the clinical pathways and on developing the IT infrastructure needed to support the pathways’ use. In contrast, Geisinger used financial incentives to encourage physicians to implement the practice infrastructure changes that were necessary for the medical home program to get off the ground.
Making integrated care work
A shift toward integrated care is usually a substantial change for a health care organization. Change often causes discomfort and confusion, and those reactions can hinder a pilot project’s success. Studies have shown that most change programs fail, and most of those failures arise from cultural factors—either senior managers are not supportive of the change or employees are resistant to it.
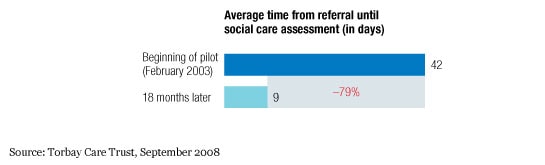
If an integrated-care pilot is to succeed, therefore, strong support for it must be developed among all participants, which is part of the reason that appropriate incentives and clinical leadership are so important. A good communication program can also help in this regard. For example, when community care and health care providers in Torbay, England, decided to integrate in 2005, the merged organization (the Torbay Care Trust) knew that it would have to offer its staff a clear rationale for change. The trust began by communicating a clear and concise vision to all staff members of how they—and their patients—would benefit from integrated care. The goal was to excite the staff about a new way of working. The trust then put a structural solution in place: it physically collocated the health and social care professionals to signal that they would collaborate from then on. Integrated care is working well in Torbay: the time until patients undergo social care assessment has decreased substantially (Exhibit 3), and the trust recently won an award for its long-term care services.
Shorter waits for social care assessments
An organization that wants to build support for an integrated-care pilot must remember, however, that enthusiasm alone is not sufficient for the pilot’s success. What is required instead is a deep transformation of attitudes and behaviors so that all participants commit themselves to integrated care and the changes it will require. Central to Kaiser Permanente’s success, for example, is the conviction among all of the system’s physicians and nurses that hospital admissions often represent a failure of care. This belief unites the staff around the common goal of keeping patients healthy.
In most parts of the world, integrated care is still a new idea, and the number of integrated-care providers is small. Thus, considerably more research is needed to determine how integrated care can best be used to improve clinical outcomes and control health care costs. However, enough organizations have had sufficient experience with integrated care to prove that it can be a highly effective way to enhance the well-being of chronically ill and elderly patients.
Related Articles
