New regulations that require US health care providers to use electronic health records (EHR) and adhere to strict data-coding standards will force hospitals to spend billions of dollars over the next decade to upgrade their IT systems. The spending requirements risk squeezing hospital capital budgets already under strain from steadily rising costs. With government incentives covering only a small portion of the total, providers will be forced to recover quickly their investment dollars from operating changes.
Our research shows that automating and standardizing health care information can bring benefits that extend beyond meeting demands for compliance. A provider that creates a best-practice IT platform to house and share medical records, to manage hospital resources more transparently, and to define precise guidelines for medically authorized tests and procedures can generate significant operating efficiencies. Such a platform minimizes paperwork, reduces the number of unnecessary treatments, and lowers the risk of drug and medical error.
The productivity and resource savings often pay back the initial IT investment within two to four years while also producing better health outcomes for patients. We estimate that total savings across the US provider landscape could be on the order of $40 billion annually. (By comparison, about $1.3 trillion a year is spent on inpatient and outpatient services across the United States and about $80 billion on health care IT.) Achieving such a positive return on investment (ROI), however, requires distinctive change-management skills among hospital leaders, better governance, and sustained engagement from key clinicians.
New regulatory standards
Estimates suggest that a wave of US legislation and regulatory changes will affect up to 80 percent of the existing hospital IT applications. Among the most far-reaching of these developments are provisions, laid down by the American Reinvestment and Recovery Act (ARRA), requiring health care providers to implement IT capabilities such as electronic health records and computerized-physician-order-entry (CPOE) systems. While some providers use electronic health records on a limited basis, the new regulations standardize what is expected from them and make their use mandatory.
An accelerated timetable means that US health care providers have until the end of 2015 to make the investments or face fines starting at $2,000 a bed in the first year and up to $35,000 a bed by 2019.1 In addition, both revisions to the Health Insurance Portability and Accountability Act (HIPAA) 5010 and the switch to ICD-10 require providers to apply strict new data-coding standards—no small task given the number of databases, hospital systems, and clinicians affected.
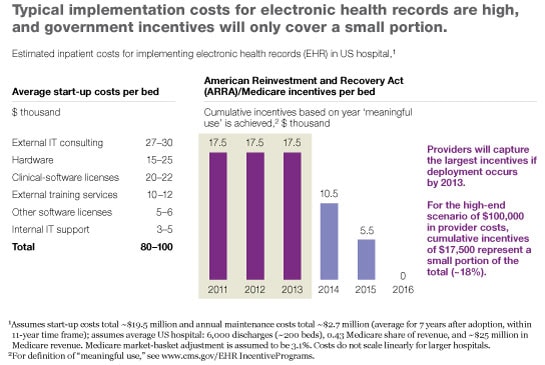
To meet these various requirements, US hospitals will need to spend approximately $120 billion, at an average cost of $80,000 to $100,000 per bed, for the required project planning, software, hardware, implementation, and training. Although the ARRA provides financial incentives under Medicare, these reimbursements offset only approximately 15 to 20 percent of total expenditures. For an average provider, the result is a spending gap of about $60,000 to $80,000 a bed (exhibit). With costs already rising by approximately 10 percent annually—and outpacing revenues—these investments will place new financial burdens on hospitals.
Where gains are possible
Many of the mandated improvements could bring wider benefits, especially in enforcing the behavioral changes needed to standardize provider practices. Electronic-health-record systems provide clinicians and other staff members with online access to patient data and decision support, such as lab reports and treatment order sets. Computerized physician order entry, a major component of those systems, requires physicians, nurse practitioners, and other specialists to follow a menu of defined procedures when requesting services, tests, or drugs for patients. Combined with clinical-decision-support (CDS) tools that give physicians best-practice guidelines for medical procedures and with stricter coding classifications, electronic health records not only broaden access to medical information but also serve as a forcing agent to spur the adoption of standard operating procedures and best medical practice.
These developments could reduce medical errors and foster better health outcomes while decreasing waste and administrative time. They could also strengthen the financial health of hospitals. Our research shows that optimizing the use of labor, reducing the number of adverse drug events and duplicate tests, and instituting revenue cycle management can help typical hospitals generate savings of some $25,000 to $44,000 per bed a year. On an industry-wide basis in the United States, this translates into $30 billion to $40 billion annually.
Electronic health records and related technologies can be applied to improve the delivery of health care in several core areas.
Optimizing the use of labor
Many hospitals continue to rely on manual charting, paper records, and outdated software to manage bed counts, schedule staff, and reserve key resources, such as operating rooms and imaging machines. Electronic health records and computerized physician order entry bring these elements together online, automating charts, records, and medical information about patients and directing medical staff toward protocols clinically proven to be more effective in treating illnesses.
When these technologies are linked to bed-management and equipment-scheduling software, doctors, nurses, and administrators can assess current and projected bed counts and optimize the scheduling of key equipment (for instance, x-ray systems) and the level of staffing. This approach reduces not only administrative waste (such as time spent tracking down medical information or calling to secure needed services) but also the level of overbooking, simultaneously improving bed turnover. The results can save upward of $20,000 per bed in labor utilization alone.
Reducing the number of adverse drug events
Electronic health records and computerized-physician-order-entry systems can sharply reduce the risk of prescription error and negative drug interactions by mapping patient histories with information from drug manufacturers to highlight the risks of prescribing a particular product. Problems with drugs cost hospitals $8,000 to $15,000 per bed each year, or between $1.6 million and $3 million for an average 200-bed hospital. Access to medical information allows physicians to adjust prescriptions or dosages to prevent complications, improve the quality of care, and reduce the human impact of adverse drug events.
Managing the revenue cycle
Every year, roughly 0.4 percent of hospital services go unbilled, at a cost per bed of just over $4,000. Some of the billing issues result from coding errors or eligibility questions. Coupled with data standards such as ICD-10, computerized-physician-order-entry systems promote the consistent naming, coding, and classification of treatments, allowing hospitals to improve the oversight of all procedures and to increase the first-time pass-through of claims.
Reducing the number of duplicate tests
When all health records are stored in electronic format and providers gain access to them through health information exchanges, they become more widely accessible to doctors, insurers, hospital administrators, and patients, regardless of location. This kind of visibility gives clinicians a more complete sense of a patient’s history and reduces the need for duplicate tests that can affect the quality, cost, and speed of care.
An average hospital can pay back its initial (and usually onetime) investment in two to four years; cost savings accrue year on year. Health care providers with better-integrated systems often realize even higher ROI.
Maximizing the potential
The realization of the benefits from health care IT investments will require a radically new approach to IT on the part of the CIOs of health care providers, as well as the business leaders and clinicians those CIOs serve. Health care providers will need to use new approaches to achieve an inclusive governance process with streamlined decision-making authority, a radically simplified IT architecture, and a megaproject-management capability.
One midsize US acute-care hospital discovered this truth when it implemented an integrated IT system designed to reduce the number of adverse drug events, improve remote access to data, and increase overall patient safety. Rather than taking a phased approach that would have allowed the IT team to factor in lessons learned as it went along, the team forged ahead on multiple fronts. Delays mounted as the hospital’s vendor struggled under the volume of the new requirements for software applications. The lack of senior-leadership direction and input from physician leaders meant that the system went live with gaps in the standard guidelines, such as basic guidance on aspirin dosages for patients with heart problems. Rather than reducing the number of adverse drug events, the new system actually raised error rates.
Three implementation stories
As the following examples show, hospitals can benefit from effectively implementing electronic health records, computerized-physician-order-entry systems, and coding standards.
An enormous gain. A regional health care provider in Canada successfully implemented electronic health records and related systems in four large hospitals. Over four years, the hospital system developed standard guidelines for medical procedures and decision support protocols, configured and implemented the new IT system, and rolled it out to the area’s four major hospitals, achieving a 90 percent-plus adoption rate by clinicians.
Although the upgrade’s cost was substantial (approximately Can $100 million), the improvements generated the same amount in annual savings by reducing labor requirements, duplicate lab tests, and adverse drug events. This achievement freed staff members to focus more time on their primary duties, a shift that allowed the hospitals to treat 20 percent more patients without an increase in personnel or reduction in quality. A 20 percent jump in productivity is an enormous gain—in a US-style health care system, that level of performance would translate into more than $100,000 per bed a year in savings. That’s far higher than our conservative ROI estimate for typical successful implementations. Moreover, the use of standardized guidelines developed by the region’s leading physicians helped spread the use of best-practice medical procedures, which improved patient outcomes. In cardiac care, for instance, patients treated with the recommended protocols healed more quickly and spent fewer days in hospitals.
Simple is better. A large health system sought to consolidate its disparate IT assets as it reorganized. The existing IT footprint was diverse, with multiple instances of similar applications, variations in capabilities across care settings, and a diverse portfolio of vendors. These problems raised operating and capital requirements and made it hard to share information across hospitals.
In planning a long-term investment strategy, the health system developed a radically simplified blueprint of its end-state IT. The focus was to migrate to a single platform for each purpose, leverage existing assets, and redirect investment toward new capabilities. By taking this approach, the health system developed a five-year investment strategy eliminating 80 percent of its existing platforms, with estimated run rate savings of 30 percent, while maintaining its historical capital-investment levels.
The benefits of planning and piloting. A large US health care provider with about 50 hospitals across multiple states sought to implement an electronic-health-record system that would achieve high acceptance among clinicians. A handpicked IT team led the project. Because this was as much an organizational-change assignment as it was an IT implementation, the team spent substantial time at the outset planning what processes should be improved, engaging frequently with leaders in the physician community to discuss expectations, and formulating a list of desired changes.
To manage complexity, the team piloted the first few rollouts so it could make improvements as it went along. This approach helped the team complete the subsequent implementation in the hospital system as a whole much more quickly than would have been possible without learning from the pilots. Training materials and change-management techniques were piloted as well to smooth the transition and encourage adoption. Although the implementation is ongoing, after the first three months this phased-in approach has already resulted in adoption levels as high as 75 percent for computerized-order-entry systems. The project is tracking close to time and budget.
Lessons of implementation
As these cases show, three success factors distinguish the best IT implementations among health care providers.
Governance with real authority. Involving key stakeholders, such as clinicians and hospital administrators, early in the IT decision process is critical to ensure buy-in and to inform requirements. To achieve the value at stake, clinicians and administrators will need to change their behavior. In many cases, this is very difficult to do.
The regional health care provider in Canada used a radical new governance model to get highly regarded physicians deeply involved as champions in the process of selecting the IT system and leading the development of guidelines for medical procedures. These physicians also helped the provider engage with the broader physician community to encourage acceptance during the implementation of the project and adoption after it was completed.
Our experience indicates that provider IT implementations of this magnitude can be successful. But they always require a step change in an organization’s approach to governance and change management, from the selection of clinician leaders and champions to the creation of governing bodies focused on specific topics (such as order set development), clear decision authority among stakeholders, and training at the point where IT systems interact.
Radical simplification of architecture. Diverse IT applications and platforms, common among providers today, create a significant degree of complexity, raise costs, and lengthen implementation time lines. The delays and cost escalation can undermine large-scale health care IT implementations. A radically simplified architecture, which eliminates the complexity and reduces the cost of large-scale system implementations, can be a critical prerequisite to success.
Methodical planning and execution. For IT to enable better clinical work flows and medical practices, many elements must come together. The implementation team should address the IT architecture, standards, and changed medical practices in the early planning stages. Implementation should be rolled out in a systematic, modular way, with active tracking of progress and lessons learned. It’s important not to underestimate the amount of time and due diligence that go into planning a megaproject.
The Canadian hospital system, for instance, allocated approximately 30 percent of its total project budget to change management—a figure that is consistent with those in other successful implementations and fits within our estimate of $80,000 to $100,000 a bed. The US health care provider rolled out its IT system in a series of phased pilots across each hospital, an approach that allowed it to capture lessons and use them in subsequent rollouts. A full-time implementation team and “war room” were established to track progress and provide support and training to physicians throughout the change process.
All successful large-scale implementations of health care provider IT systems have used similar sophisticated megaproject-management approaches.
Over the next decade, costs and regulatory mandates will require providers to make significant new investments in health care IT. Given the value at stake, hospital management will be under pressure to demonstrate an appropriate return for every dollar spent. Hospitals that take a systemwide approach to overhauling IT—a governance model with real authority, a radically simplified IT architecture, and a robust megaproject-management methodology—will be well positioned not only to meet their compliance responsibilities but also to lower their operating costs significantly while improving the quality of patient care.

